
By Baher Ibrahim
This post was originally published on Baher Ibrahim’s Substack “Migrant Psychiatrist”.
‘The gallows in my garden, people say,
Is new and neat and adequately tall;
I tie the noose on in a knowing way
As one that knots his necktie for a ball;
But just as all the neighbours–on the wall–
Are drawing a long breath to shout “Hurray!”
The strangest whim has seized me. . . . After all
I think I will not hang myself to-day.’
— G.K. Chesterton, A Ballade of Suicide1
Suicide between the wish to kill and the wish to die
On one of my first ever ward rounds as a resident psychiatrist, I was following around a very senior and experienced consultant who I did not know well but whose empathy and humanism I will never forget. A woman was in hospital for the purposes of maintaining her safety. She had had an argument with her partner, who stormed out of their home and did not return that night. She assumed he was out on another drinking binge, until two days later when an early morning jogger found his body hanging from a tree by the mighty River Clyde. This Clyde suicide has stayed with me since that day. The shock, grief, bewilderment, anger, and shame are impossible to truly understand and I will not pretend to. Instead, I will direct the reader to r/SuicideBereavement, whose narratives make for harrowing reading. The doctor I was shadowing listened more than he talked, and acknowledged what the woman was feeling and thinking: that the feeling of loss she was experiencing would never truly go away, even as it became more manageable with the passage of time. This woman was asked if she was experiencing suicidal thoughts. She responded that she was, but that she would never do something like that to her children.
I had just moved into psychiatry after a placement on a palliative care ward, where conversations around Do Not Attempt Resuscitation (DNAR) orders were commonplace and expected. That ward was populated by terminally ill patients who did not want to prolong their suffering — if they went into a cardiac arrest, they were happy to die. Other patients, or their family members, asked us to speed up their dying process, a request that was illegal to comply with. These people also wanted to die. For a split second that day when shadowing the consultant, I imagined his question about whether she wanted to die was the beginning of a DNAR conversation, before realizing this was a suicide ‘risk assessment’. This woman was angry and in immense emotional pain, but she did not want to die. She did not have a death wish.
American psychiatrist and psychoanalyst Karl Menninger wrote that the act of suicide fulfils three wishes: the wish to kill, the wish to be killed, and the wish to die.2 The first of these embodies the desire to discharge an aggressive impulse through violence, in this case against oneself; the second embodies the desire to destroy a part of the self that the person despises and finds alien; and the third signifies the desire to stop living. All three need to be present for a suicide to be completed. In three and a half years of working as a psychiatrist, only three people I interacted with in my clinical work died by suicide within weeks of my contact with them. None of them had expressed a recent intent to kill themselves. All of them had reassured their doctors that they felt safe. Two of them were clearly premeditated — an overdose in a hotel room of an undisclosed location to avoid discovery and hanging oneself from the loft soon after discharge from hospital. The third almost certainly had not planned to die — this was the umpteenth overdose in a supported living facility with regular staff checks, but on this day the shift was busy and the staff did not get to her in time. This is what is referred to in the clinical record as ‘misadventure’.
The language and philosophy of suicide
The reader will note that I have used the phrases ‘die by’ and ‘completed’ suicide rather than the better known ‘commit suicide’. Few good things follow the word ‘commit’ — humans commit murder and fraud, but they don’t commit charity and benevolence (they can also commit to another person, but this begs the question of whether committing wholly to another human being in a romantic relationship is a good thing). For most of history, suicide was a sin in religion and a crime in law. The word suicide comes from the Latin sui (of oneself) and cīdium (killer/killing). The suffix –cide is common in words signifying some sort of killing: pesticide, insecticide, regicide, genocide. While the word ‘suicide’ per se has not become similarly stigmatized, internet algorithm censorship has prompted Gen Z to come up with abbreviations or neologisms: to ‘kms’ (kill myself) or ‘unalive’ oneself. The latter has crept into clinical practice.
Although ‘commit’ has fallen out of favor, ‘suicidal’ as an adjective enjoys great popularity. It is never clear if ‘suicidal’ refers to thoughts, emotions, behaviour, or something else. Many have learned through trial and error that the strategy to raise risk perception among loved ones, carers, and clinicians is to declare that one is ‘suicidal’. It is often the surefire way to gain admission to a psychiatric ward, if this is what someone wants. It is supposed to fall to psychiatrists to understand what this means. Many are unable or unwilling to elaborate when they are in a state of extreme distress — ‘I told you I was suicidal, what more do you need to know?’ or ‘I can’t keep myself safe if that’s what you are asking’. The word suicide is supposed to do the emotional heavy lifting.
Saying one is suicidal actually says very little. It is about as enlightening as saying one is ‘hungry’. One does not walk into a restaurant and say they are hungry without further elaboration. What do they want to eat? Do they want to eat it now? Does the restaurant have what they want to eat? Will they accept what the restaurant does have? Do they have any dietary restrictions? Are they prepared to pay the price for what is on offer? And so on.
Similarly, those who present to mental health services in suicidal crises can struggle to contextualize their suicidal feeling. Are they suicidal in a philosophical sense like Albert Camus who believed that suicide was the only philosophical question worth asking?3 Are they wanting to die because their life is meaningless and they cannot bear it; and, if so, are they able to create some of the desired meaning? Do they have a terrible quality of life that makes death preferable; and, if so, is there anything that can be done to make them feel otherwise? Did they only become suicidal today? If so, what happened; and if not, what has changed today? Is the reason they want to die, or kill themselves, something that a psychiatrist has any power to change?
The invention of ‘suicidality’ as communication strategy
A pillar of training in the mental health professions is responding to and managing people in distress who present in a suicidal crisis. Among the most fascinating cohort of patients are those who have attracted a label of borderline personality disorder or emotionally unstable personality disorder. This is also the patient group that was described in a communication by the Royal College of Psychiatrists as a ‘thorn in the flesh of many clinicians’, both for the resources consumed by their issues and for the feelings of dissatisfaction and helplessness they engender in clinicians. When these patients are asked some of the above questions in a state of crisis, they can feel alienated, misunderstood, and not taken seriously. They can feel that anything other than the clinician acceding to the immediate demand — of medication or hospital admission — means that they do not care about them. They can also feel that the only way to demonstrate distress is by self-harm or threats of suicide. They can also feel that if they accept an offer of admission to hospital, they appear to not really want to die. It must come from the doctor who makes a unilateral decision to enact a coercive and nonconsensual measure of detention under the Mental Health Act — this shows that the doctor cares enough to detain them, and it shows to their family that they are so unwell that the doctor had no choice but to detain them.
This tying of a person’s intentions and emotions to visible actions is called teleological thinking in one mode of therapy. One’s intentions and emotions are only real if they are manifested as the visible desired action. Some clinicians and researchers consider the chronic suicidal communications, or suicidality, of borderline PD to be so different from the ‘usual’ suicidality that they will exclude them from research studies so as not to skew the results.4
The Oxford English Dictionary tells us that the word ‘suicide’ was used as early as the seventeenth century, and ‘suicidal’ as early as the eighteenth. ‘Suicidality’, defined as ‘the fact or condition of being suicidal; inclination towards suicide’ only dates to the 1960s. My own untested theory about this is that humans adapted their expressions of distress via suicide to fit the changing context of deinstitutionalization and the advent of outpatient and community psychiatric services. These new venues offered a place that one could go to or be taken to because they are in an ongoing state of wanting to kill themselves. The presence of this new solution allowed the construction of suicidality as a problem needing an intervention as opposed to suicide as something that you either do or don’t; a problem that cannot be ignored; transforming suicide from a philosophical problem or a final act into a communication strategy. By declaring that one is suicidal, the person on the receiving end is implicated: they must act. The people who engage in what can appear to be a sort of strategic suicidality know this well. This is not to say they are consciously and maliciously manipulating another person (though they might be) but the effect on the other person of this communication is to feel manipulated and coerced. The only way to respond is counter-coercion. This is the job of the psychiatrist. The profession must also bear its responsibility for encouraging communications of this sort — we are bombarded with messages of how we should ‘reach out’ and that it is ‘okay to not be okay’. While well-intentioned, this messaging has set high expectations that cannot be fulfilled. There is no treatment for suicidality the way there is treatment for sepsis. But at least it ensures a continuous stream of patients for the profession.
A psychiatrist in professional practice within an institution cannot have an earnest conversation about suicide with a patient. They are professionally mandated to approach the issue from the premise that suicide is bad and wrong, and that the person must be dissuaded from it. Nobody has discussed this problem better than Thomas Szasz. In his book The Ethics of Psychoanalysis: The Theory and Method of Autonomous Psychotherapy, he compares his psychotherapeutic practice to agreeing to play a game of bridge. If the patient calls in between appointments and says he wants to kill himself, this is as if he is asking to change the rules of the game that were agreed upon, or to switch the game from bridge to poker. In the epilogue of the book he provides advice to therapists, such as ‘do not let yourself be coerced by “emergencies”’.5 Elsewhere he puts it more bluntly, as in his book The Second Sin — ‘“attempted suicide” is strategic psychiatric rhetoric; in most cases “attempted suicide” is actually “pretended suicide.”6 He was known for not mincing his words, and while they may come across as harsh, I am of the opinion that they came from a place of respect for the autonomy and dignity for the individual.
I am very fond of Szasz’s response to a fellow psychiatrist who asked him in a conference what he would do if a patient called in between appointments saying they wanted to kill themselves, with which I will conclude. I recommend listening to the full clip, but the core of the answer is that he would offer the person an appointment and discuss suicide with the same earnestness that he would bring to a discussion about marriage or divorce or any other big decision. Suicide is a momentous decision not to be taken lightly, and ‘you can only do it once, if you do it right’. This discussion can only take place if a number of conditions are fulfilled: the patient has turned up voluntarily to discuss his existential predicament, he genuinely wants the opinion of another person in order to inform his own decision, there is no threat of coercing the patient into doing or not doing something via the Mental Health Act, and there is no threat of coercing the psychiatrist into doing or not doing something through professional sanctions and threats to livelihood. These conditions are absent from psychiatric training and institutional psychiatric practice. For this reason, those who are curious about the human condition and seek to take people seriously, with respect for their dignity, liberty, autonomy; should not expect to realize these aspirations in psychiatry.
- G.K. Chesterton, A Ballade of Suicide.
- Karl Menninger, Man Against Himself (1938).
- Albert Camus, The Myth of Sisyphus (1942).
- Hines, Christopher E., Scott Mooney, Nora L. Watson, Stephen W. Looney, and David J. Wilkie. “Repetitive transcranial magnetic stimulation promotes rapid psychiatric stabilization in acutely suicidal military service members.” The journal of ECT 38, no. 2 (2022): 103-109.p.218
- p.218
- p.68
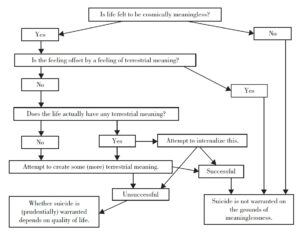
‘An example of what an earnest conversation about suicide might look like. From philosopher David Benatar’s The Human Predicament, p. 194‘
About the author
Baher Ibrahim is a psychiatrist and historian based in Scotland. He writes at migrantpsychiatrist.substack.com.